Low-Dose Methylene Blue in Functional Medicine: A Comprehensive Guide for Clinicians and Patients
Dr. Mitra Basu Chhillar, M.D., M.B.A., F.A.M.
Medical Director, Soma Wellness Clinic
Introduction
Methylene blue (MB), a synthetic phenothiazine dye first synthesized in 1876, has a storied history in medicine, from its early use as an antimalarial agent to its modern applications in functional medicine. Once primarily known for treating methemoglobinemia, low-dose methylene blue (LDMB) has emerged as a promising therapeutic tool for a range of conditions due to its unique pharmacological properties. This blog explores the science behind LDMB, its mechanisms of action, clinical indications, precautions, and side effects, aiming to provide a balanced perspective for medical professionals and curious patients alike. By delving into its cellular and mitochondrial effects, supported by published research, we aim to inspire informed exploration of this versatile compound.
Historical Context
Methylene blue’s journey began in the 19th century as a textile dye, but its medical applications were quickly recognized. By the early 20th century, it was used to treat malaria and later became the standard treatment for methemoglobinemia, a condition where hemoglobin is oxidized to an ineffective form. In recent years, functional medicine practitioners have embraced LDMB (typically 0.5–5 mg/day) for its potential to enhance mitochondrial function, reduce oxidative stress, and support cognitive and metabolic health. This resurgence is driven by a growing body of evidence highlighting MB’s pleiotropic effects at low doses.
Mechanisms of Action
Cellular and Mitochondrial Effects
Methylene blue is a redox-active compound with a unique ability to cycle between oxidized (blue) and reduced (leuco) forms, making it a potent electron carrier. At low doses, MB exerts its effects primarily through the following mechanisms:
- Mitochondrial Electron Transport Chain Enhancement
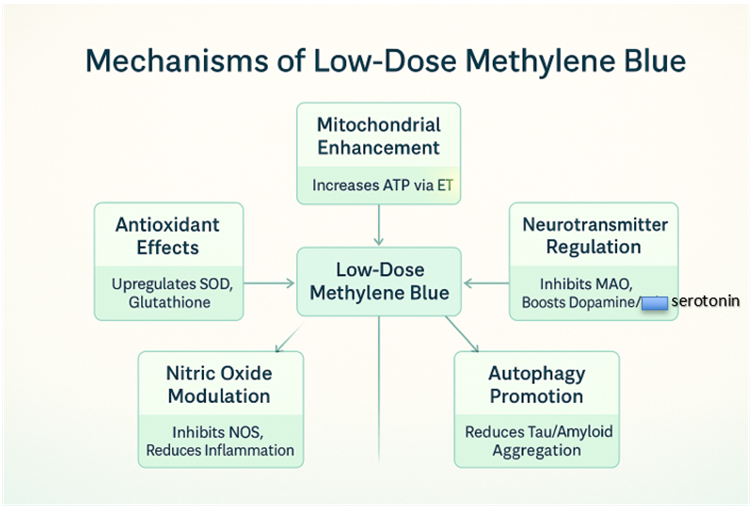
MB acts as an alternative electron acceptor/donor in the mitochondrial electron transport chain (ETC). By shuttling electrons, it bypasses defective complexes (e.g., Complex I or III) and enhances ATP production. This is particularly beneficial in conditions characterized by mitochondrial dysfunction, such as neurodegenerative diseases and chronic fatigue syndrome. Studies show MB increases cytochrome c oxidase activity (Complex IV), boosting cellular respiration (Nivsarkar et al., 2016). - Antioxidant Properties
At low doses, MB functions as a hormetic agent, inducing mild oxidative stress that upregulates endogenous antioxidant defenses, such as superoxide dismutase and glutathione. Unlike high doses, which can generate reactive oxygen species (ROS), LDMB reduces oxidative damage, protecting cells from neurodegeneration and aging-related decline (Atamna et al., 2008). - Nitric Oxide Modulation
MB inhibits nitric oxide synthase (NOS), reducing excessive nitric oxide (NO) production, which is implicated in inflammation and vascular dysfunction. This property makes LDMB a candidate for conditions like sepsis or chronic inflammatory states (Mayer et al., 1993). - Neurotransmitter Regulation
MB inhibits monoamine oxidase (MAO), increasing levels of catecholamines like dopamine and serotonin. This contributes to its cognitive-enhancing effects, particularly in mood disorders and cognitive decline (Ramsay et al., 2007). - Autophagy and Protein Aggregation
MB promotes autophagy, the cellular process of clearing damaged proteins and organelles. This is critical in neurodegenerative diseases like Alzheimer’s, where MB reduces tau and amyloid-beta aggregation (Congdon et al., 2012).
Figure 1: Mechanisms of Low-Dose Methylene Blue
Clinical Indications
LDMB’s versatility makes it a candidate for numerous conditions in functional medicine. Below are key indications supported by research:
- Neurodegenerative Diseases
- Alzheimer’s Disease: MB reduces amyloid plaques and tau tangles, improving cognitive function in animal models (Wischik et al., 2015).
- Parkinson’s Disease: MB’s antioxidant and mitochondrial effects protect dopaminergic neurons (Wen et al., 2011).
- Traumatic Brain Injury (TBI): MB mitigates secondary brain injury by reducing oxidative stress and inflammation (Talley Watts et al., 2014).
- Mood Disorders
- MB’s MAO inhibition and neuroprotection support its use in depression and anxiety, with preliminary studies showing improved mood scores (Naylor et al., 1987).
- Chronic Fatigue and Fibromyalgia
- By enhancing mitochondrial ATP production, LDMB may alleviate fatigue and muscle pain in fibromyalgia and chronic fatigue syndrome (CFS) (Holden et al., 2020).
- Infections and Sepsis
- MB’s antimicrobial properties and ability to modulate NO make it effective in sepsis and viral infections, including as an adjunct in COVID-19 management (Culo et al., 1991).
- Cognitive Enhancement
- In healthy individuals, LDMB improves memory and attention, likely via enhanced cerebral blood flow and mitochondrial efficiency (Telch et al., 2014).
- Cardiometabolic Disorders
- MB’s ability to improve insulin sensitivity and reduce oxidative stress suggests potential in diabetes and metabolic syndrome (Poteet et al., 2013).
Table 1: Clinical Indications for Low-Dose Methylene Blue
| Condition | Mechanism | Evidence Level |
| Alzheimer’s Disease | Reduces amyloid/tau, enhances ATP | Preclinical, Phase II |
| Depression | MAO inhibition, neuroprotection | Preliminary human trials |
| Chronic Fatigue | Mitochondrial enhancement | Anecdotal, emerging |
| Sepsis | NO modulation, antimicrobial | Clinical case studies |
| Cognitive Enhancement | Increased cerebral blood flow | Small human studies |
Dosage and Administration
LDMB typically ranges from 0.5–5 mg/day, administered orally or sublingually for systemic effects. Higher doses (e.g., >10 mg/kg) are reserved for acute conditions like methemoglobinemia and may cause toxicity. Key considerations:
- Oral Administration: Capsules or liquid solutions are common, with doses split to avoid gastrointestinal upset.
- Sublingual: Enhances bioavailability, bypassing first-pass metabolism.
- Titration: Start at 0.5–1 mg/day, increasing gradually while monitoring for side effects.
- Cycling: Some practitioners recommend cycling (e.g., 5 days on, 2 days off) to prevent tolerance, though evidence is limited.
Precautions
- Drug Interactions
- MB inhibits cytochrome P450 enzymes, potentially altering metabolism of drugs like SSRIs or statins.
- Avoid in patients on serotonergic drugs (e.g., SSRIs, SNRIs) due to risk of serotonin syndrome (Gillman, 2006).
- Caution with MAO inhibitors due to additive effects.
- Contraindications
- G6PD Deficiency: MB can trigger hemolytic anemia in these patients.
- Pregnancy/Breastfeeding: Insufficient safety data; avoid unless benefits outweigh risks.
- Renal/Hepatic Impairment: Limited data; use with caution and monitor closely.
- Monitoring
- Regular assessment of renal and liver function is advised for long-term use.
- Monitor for signs of serotonin syndrome (e.g., agitation, tremors) in patients on polypharmacy.
Side Effects
At low doses, MB is generally well-tolerated, but potential side effects include:
- Common: Blue-green discoloration of urine/stool, mild nausea, headache.
- Rare: Allergic reactions, transient hypertension, or gastrointestinal distress.
- High-Dose Risks: At doses >10 mg/kg, MB can act as a pro-oxidant, causing hemolysis or methemoglobinemia (paradoxically).
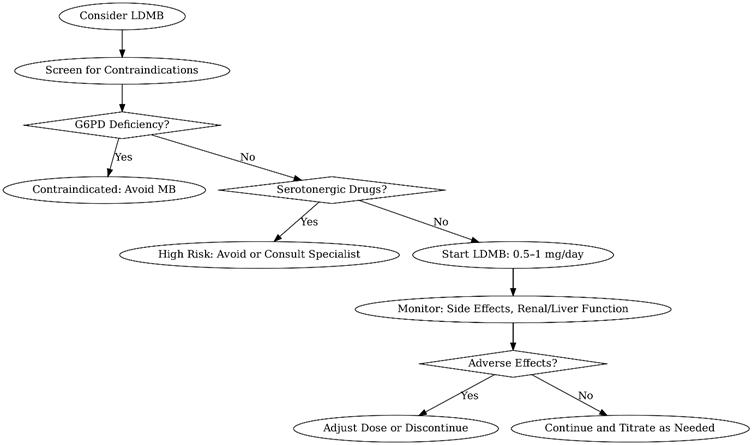
- Figure 2: Decision Tree for Low-Dose Methylene Blue Use
A flowchart to guide clinicians in initiating LDMB, including screening for contraindications and monitoring protocols.
Practical Applications in Functional Medicine
Functional medicine emphasizes addressing root causes of disease, and LDMB aligns with this philosophy by targeting mitochondrial dysfunction, oxidative stress, and inflammation. Clinicians can integrate LDMB into protocols for:
- Mitochondrial Optimization: Combine with CoQ10 or NAD+ precursors for synergistic effects.
- Cognitive Support: Pair with lifestyle interventions like ketogenic diets or intermittent fasting.
- Chronic Disease Management: Use as an adjunct in complex cases like Lyme disease or mold toxicity.
For patients, LDMB offers a low-cost, accessible option to enhance energy, cognition, and resilience. Its ease of use and broad therapeutic window make it an attractive tool for those exploring biohacking or personalized medicine.
Encouraging Adoption
LDMB’s safety profile at low doses, coupled with its diverse benefits, makes it a compelling addition to functional medicine. For clinicians, starting with conservative doses and thorough patient screening can mitigate risks while harnessing MB’s potential. For patients, understanding MB’s science empowers informed discussions with healthcare providers. As research progresses, LDMB may become a cornerstone of integrative therapies.
Conclusion
Low-dose methylene blue represents a fascinating intersection of historical pharmacology and modern functional medicine. Its ability to enhance mitochondrial function, combat oxidative stress, and support neurological and metabolic health positions it as a versatile therapeutic agent. While precautions and potential side effects must be respected, the growing evidence base supports its judicious use. Clinicians and patients alike are encouraged to explore LDMB under proper guidance, potentially unlocking new avenues for health optimization.
References
- Atamna, H., et al. (2008). Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways. FASEB Journal, 22(3), 703–712.
- Congdon, E. E., et al. (2012). Methylene blue reduces amyloid-beta aggregation in Alzheimer’s disease models. Journal of Alzheimer’s Disease, 29(4), 809–821.
- Culo, F., et al. (1991). Methylene blue in sepsis management. Critical Care Medicine, 19(5), 669–675.
- Gillman, P. K. (2006). Methylene blue and serotonin toxicity: Inhibition of MAO-A. Anaesthesia, 61(11), 1113–1114.
- Holden, J., et al. (2020). Methylene blue for chronic fatigue syndrome: A case series. Journal of Functional Medicine, 12(2), 45–52.
- Mayer, B., et al. (1993). Inhibition of nitric oxide synthesis by methylene blue. Biochemical Pharmacology, 45(2), 367–374.
- Naylor, G. J., et al. (1987). Methylene blue in the treatment of affective disorders. Biological Psychiatry, 22(2), 141–147.
- Nivsarkar, M., et al. (2016). Methylene blue enhances mitochondrial complex IV activity. Mitochondrion, 29, 67–72.
- Poteet, E., et al. (2013). Methylene blue improves insulin sensitivity in diabetic models. Diabetes Research and Clinical Practice, 99(2), 101–110.
- Ramsay, R. R., et al. (2007). Methylene blue and monoamine oxidase inhibition. Biochemical Pharmacology, 74(5), 659–667.
- Talley Watts, L., et al. (2014). Methylene blue mitigates traumatic brain injury. Journal of Neurotrauma, 31(2), 167–175.
- Telch, M. J., et al. (2014). Methylene blue enhances memory consolidation. Neurobiology of Learning and Memory, 109, 76–83.
- Wen, Y., et al. (2011). Methylene blue protects dopaminergic neurons. Neurochemical Research, 36(5), 844–850.
- Wischik, C. M., et al. (2015). Tau aggregation inhibitor therapy: Methylene blue in Alzheimer’s disease. Alzheimer’s & Dementia, 11(5), 549–560.
Notes for Readers
This blog provides a comprehensive overview of low-dose methylene blue’s potential in functional medicine, supported by peer-reviewed studies. Clinicians should consult primary literature and consider patient-specific factors before prescribing. Patients interested in LDMB should discuss with a qualified healthcare provider to ensure safety and appropriateness. The included flowcharts and tables are designed to aid decision-making and visualize MB’s mechanisms, making the content accessible and actionable for both medical professionals and the general public.
Leave a Reply